How To Check Nasogastric Tube Placement

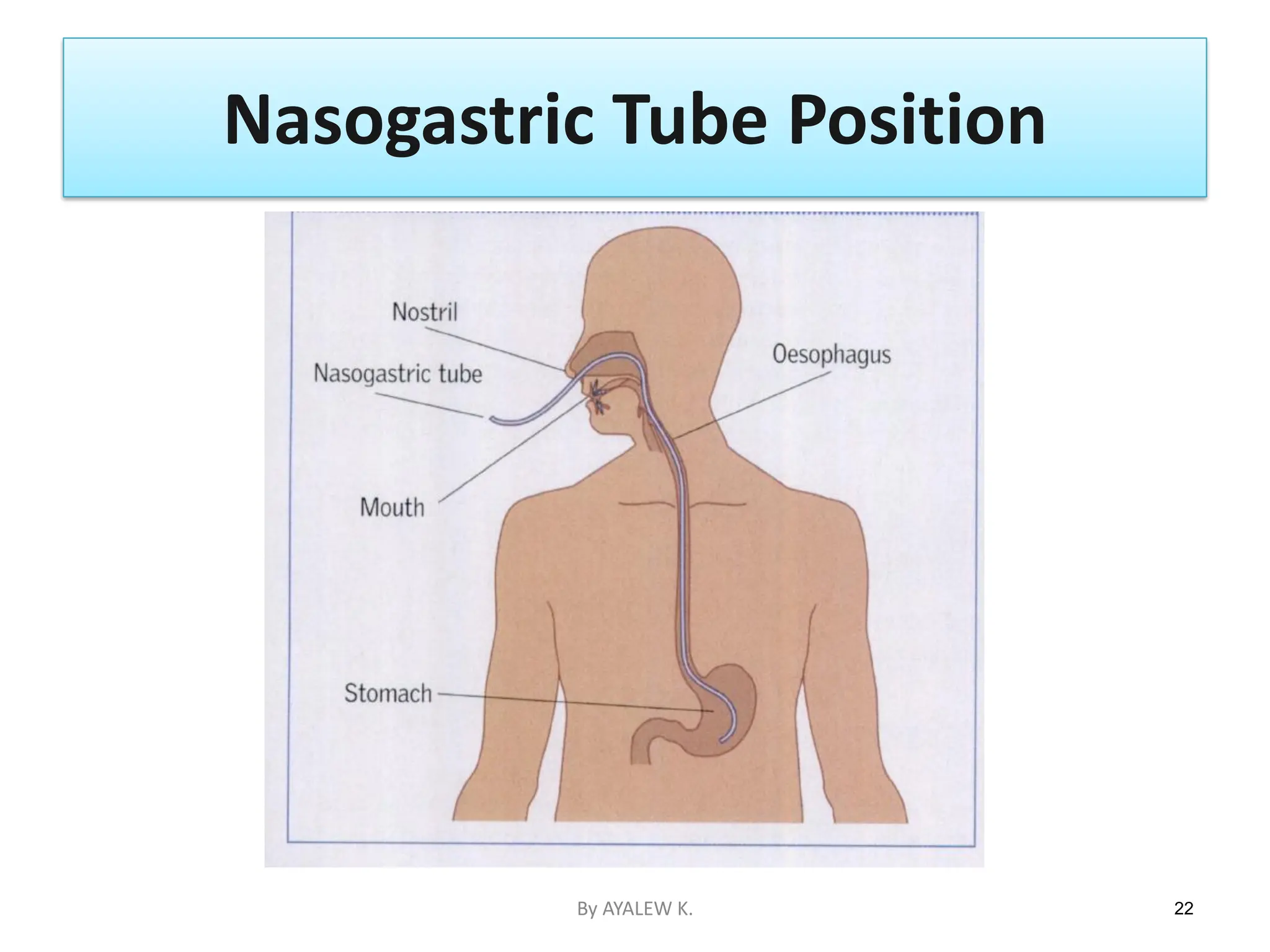
Alright, buckle up, fellow adventurers in the land of healthcare! Today, we're diving headfirst (pun intended!) into a topic that might sound a tad intimidating, but I promise, it's as straightforward as making a perfect peanut butter and jelly sandwich. We're talking about checking if a nasogastric tube, or as I like to call it, the trusty NG tube, is exactly where it's supposed to be. Think of it like making sure your GPS is locked onto the right destination before you embark on a grand road trip. We want that tube in the tummy, folks, not chilling in the lungs where it has absolutely no business being!
Imagine this: you've got this super important delivery truck, the NG tube, carrying precious cargo (like medicine or nutrients) all the way to the stomach. If that truck accidentally takes a wrong turn and ends up in the respiratory highway, well, that's a recipe for a bit of a traffic jam, and nobody wants that! So, our mission, should we choose to accept it (and we totally do!), is to do a quick and easy peek to confirm our delivery truck is on the right track. It's all about ensuring comfort, safety, and that our patient is getting exactly what they need, precisely where they need it. No detours allowed!
First things first, let's talk about the secret weapon in our arsenal: gastric aspirate. This is basically like taking a tiny peek inside the stomach to see what's cooking. We're looking for a nice, clear, greenish-brown liquid. Think of it as the stomach's very own special sauce. If you get something that looks like clear water, or even worse, like lung juice (which is a big no-no!), then we know something's up. It's like checking if your lemonade has the right amount of tartness – you just know when it's off!
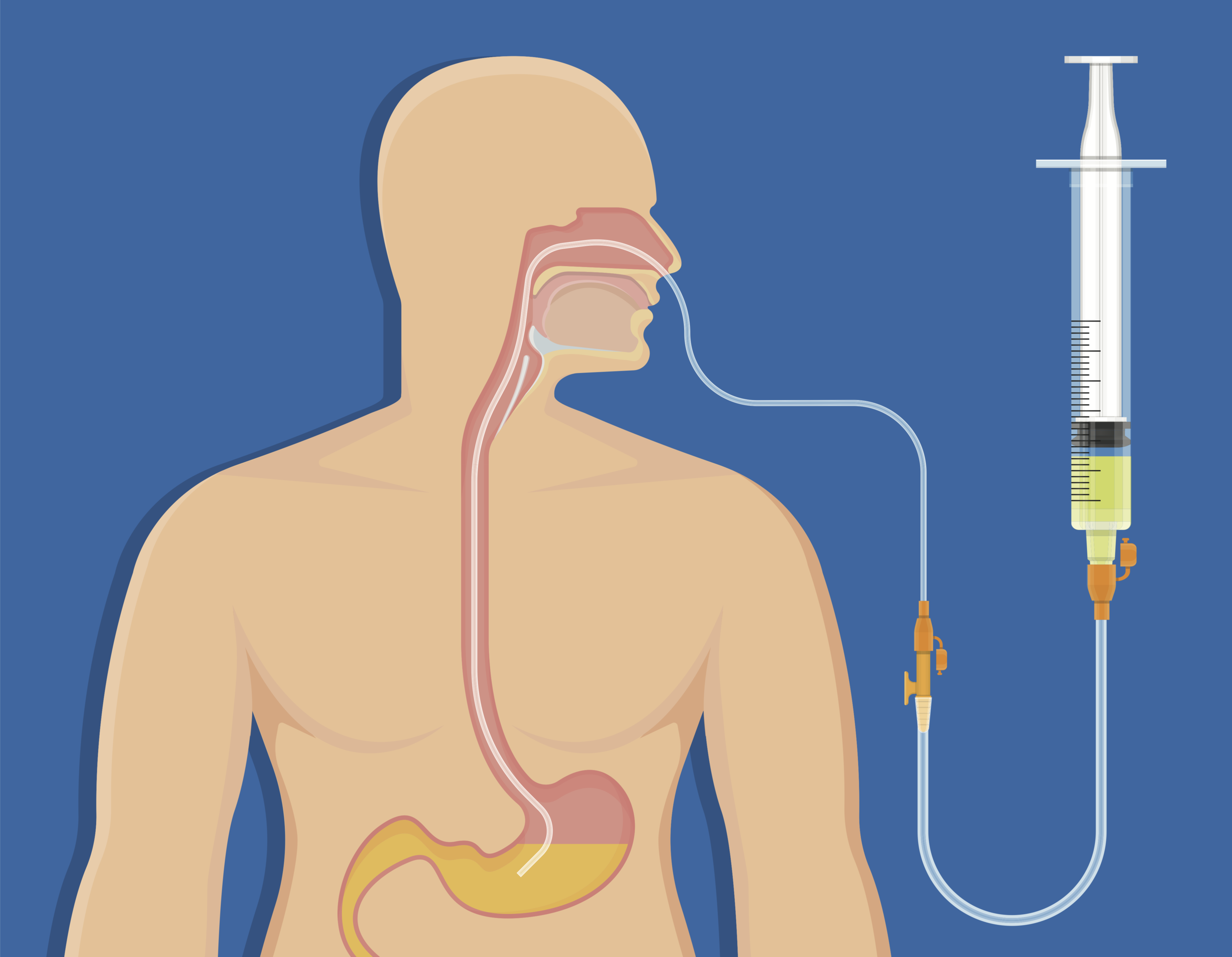
Now, how do we get our hands on this "special sauce"? It's super simple! We grab ourselves a trusty syringe. These are the unsung heroes of so many healthcare tasks, and checking NG tube placement is no exception. You'll want a good-sized one, like a 60 mL syringe, because it gives you a nice, smooth pull. Think of it like using a bigger straw to slurp up your milkshake – much more effective, right? You gently attach this syringe to the end of the NG tube. It's like connecting the hose to the faucet; a snug fit is key!
With the syringe attached, you're going to give it a gentle pull. Don't go yanking like you're trying to win a tug-of-war! We're aiming for a calm, steady motion. If you feel a bit of resistance, that's a good sign! It means you're likely in the stomach, where things are a little more… substantial. Imagine trying to pull water from a well – you feel that satisfying tug as the bucket fills. That's the feeling we're going for!
Pro Tip Alert! Sometimes, if the patient has just had a big meal, the aspirate might be a little thicker. Don't panic! It's just the stomach working its magic. Still, the color should give you a clue. Greenish-brown is our friend!
So, you've pulled back on the syringe, and out comes that lovely, greenish-brown liquid. Fantastic! That's your green light! You can then assess the pH. Now, I know "pH" sounds science-y, but think of it like a sourness scale. Stomach contents are usually quite acidic, with a pH of 5.5 or lower. We use little strips, almost like litmus paper for your tongue, to check this. Dip the liquid onto the strip, wait a jiffy, and behold! If it's in the acidic zone, you're practically singing "Hallelujah!" because that tube is definitely in the right place.
What if you pull and get… nothing? Or even worse, what if it looks clear like water? This is where we pump the brakes, folks. A clear aspirate, especially if it’s colorless, might be a sign that the tube has drifted up into the esophagus or even the lungs. That’s our giant STOP sign. In this scenario, you absolutely do NOT proceed with feeding or giving medication through the tube. It’s like seeing a red flag at the beach – you don't go swimming there!
Another super simple yet effective method is to listen. Yes, you read that right, listen! We grab a stethoscope – that cool doctor's gadget that makes your heartbeat sound like a drum solo. Then, we inject a little bit of air, maybe about 10 mL (think of it as a tiny puff of encouragement), into the NG tube while placing the stethoscope over the upper left side of the patient's abdomen. If you hear a "whoosh" or a "gurgle," like a tiny, happy stomach party, then bingo! The air has entered the stomach, and the tube is where it belongs. It’s the stomach’s way of saying, "Thanks for the air, friend! I’m here and ready for action!"
If you inject the air and hear… crickets? Or perhaps a faint bubbling sound way up in the chest area? That’s our cue to be extra cautious. It's like trying to whisper a secret to someone and hearing it echo back from across the room – something’s not quite right with the transmission!
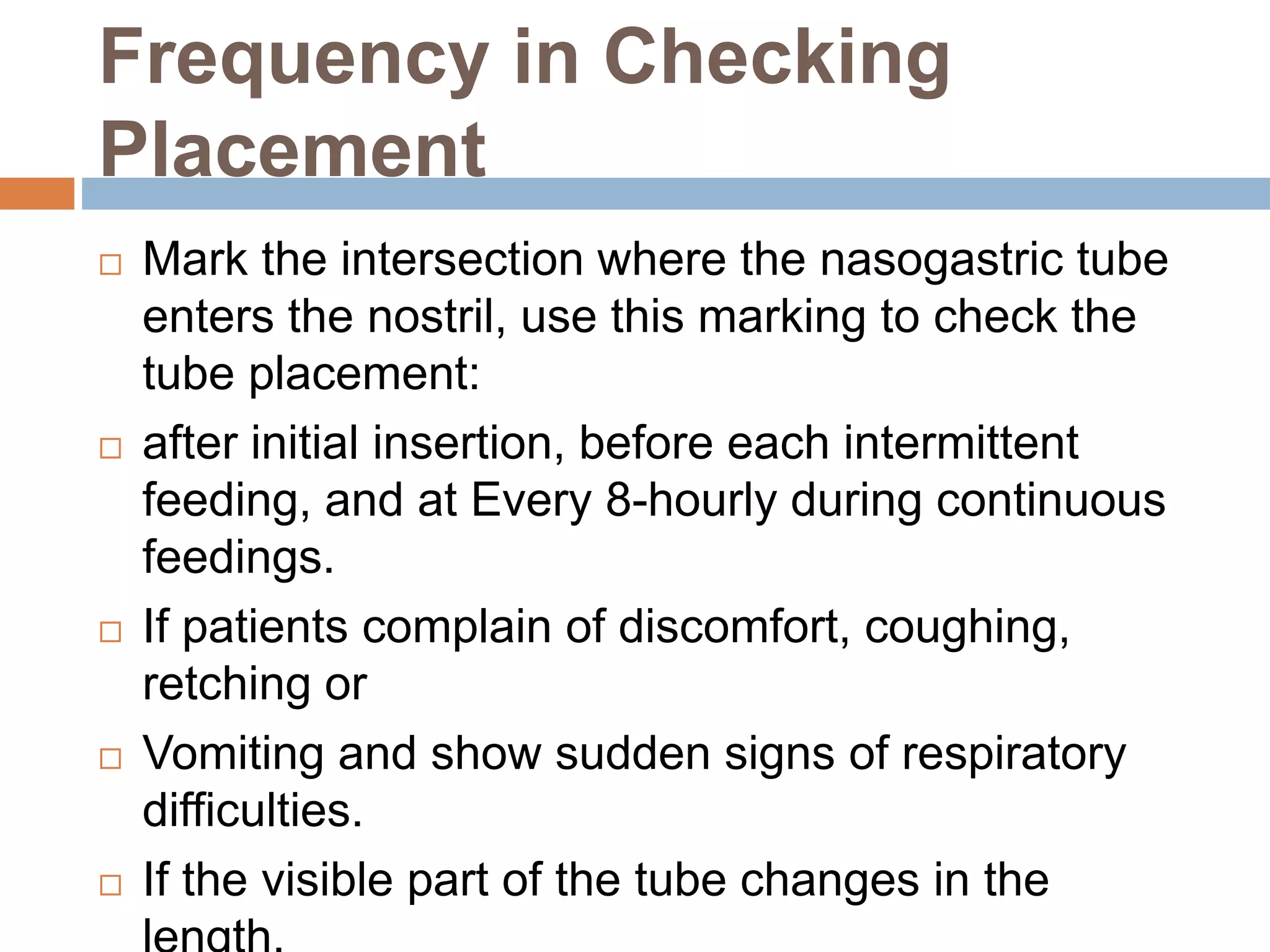
And of course, we always, always, always check the external markings on the tube itself. This is like checking the serial number on a valuable piece of equipment. You measure how much of the tube is sticking out of the patient's nose and compare it to what was documented the last time it was checked. If those numbers are drastically different, it’s like finding a clue in a mystery novel – it suggests something has moved!
So there you have it! Checking an NG tube placement isn't some arcane ritual reserved for super-geniuses. It's a straightforward process involving a syringe, a stethoscope, a keen eye for color, and a listening ear. It’s about being a detective for your patient's well-being, ensuring that vital cargo reaches its intended destination safely and soundly. You’ve got this, and your patients will thank you for it, even if they can't tell you in words. Keep up the amazing work, you healthcare superheroes!