Normal Gastric Residual Volume For Tube Feeding
I remember my first week as a brand new nurse. I was a ball of nervous energy, armed with textbook knowledge and a severe case of imposter syndrome. My patient, bless her heart, was a sweet elderly lady recovering from surgery, and she needed some supplemental tube feeding. Now, in nursing school, we learned about things like "strict intake and output" and "monitoring vital signs," but the practicalities of feeding someone via a tube? That felt like a whole different beast.
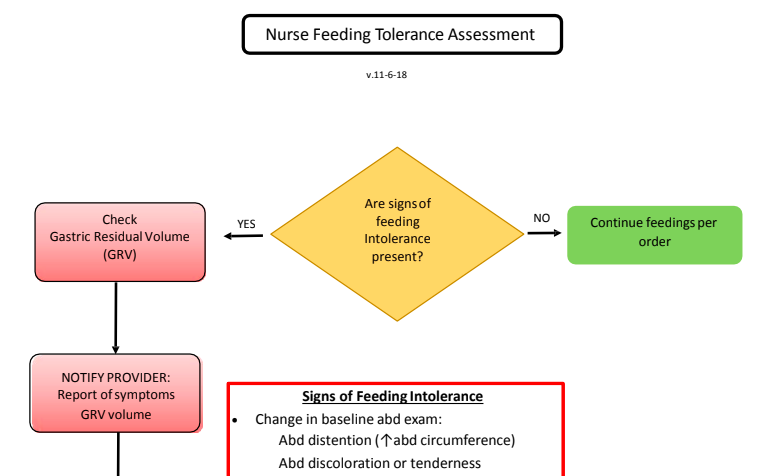
One of the things that consistently made me sweat was checking something called "gastric residual volume," or GRV. The doctor's orders would say, "Check GRV before each feeding." So, I'd grab my syringe, and… well, let’s just say some days it felt like I was trying to siphon out the entire ocean. Other days, it was like a gentle trickle. I’d stare at the amount collected, then stare at the syringe, then stare at the chart, a little knot of anxiety tightening in my stomach. Was this amount good? Was it bad? Was I about to send my patient into a feeding-induced panic? The nurses around me seemed so nonchalant, so I’d just quietly log the number and move on, hoping for the best. If only I’d had a friendly guide back then, someone to say, "Hey, it's okay, here's the lowdown on GRV!"
And that, my friends, is exactly what we're going to do today. We’re going to demystify this whole "gastric residual volume" thing. Because, let’s be honest, it sounds a bit like something you'd find in a science lab, right? But it’s actually a really important part of making sure tube feeding is safe and effective for people who need it. So, grab your favorite beverage (non-tube-fed, I hope!), settle in, and let's have a chat.
What Exactly Is Gastric Residual Volume?
Okay, let’s break it down. Imagine your stomach as a stretchy bag that holds the food you eat. When you eat, your stomach digests it, breaking it down and sending it along its merry way to the intestines. Pretty straightforward, right?
Now, for people who are receiving tube feedings, their stomach might not be emptying as efficiently as it should, or maybe they have a condition that makes them more prone to reflux. So, before we give them more food via the tube, we want to check what’s already in their stomach. That’s where the GRV comes in.
Simply put, Gastric Residual Volume (GRV) is the amount of liquid that remains in the stomach when a feeding tube is in place. It’s like a peek into your stomach’s current "fullness" level.
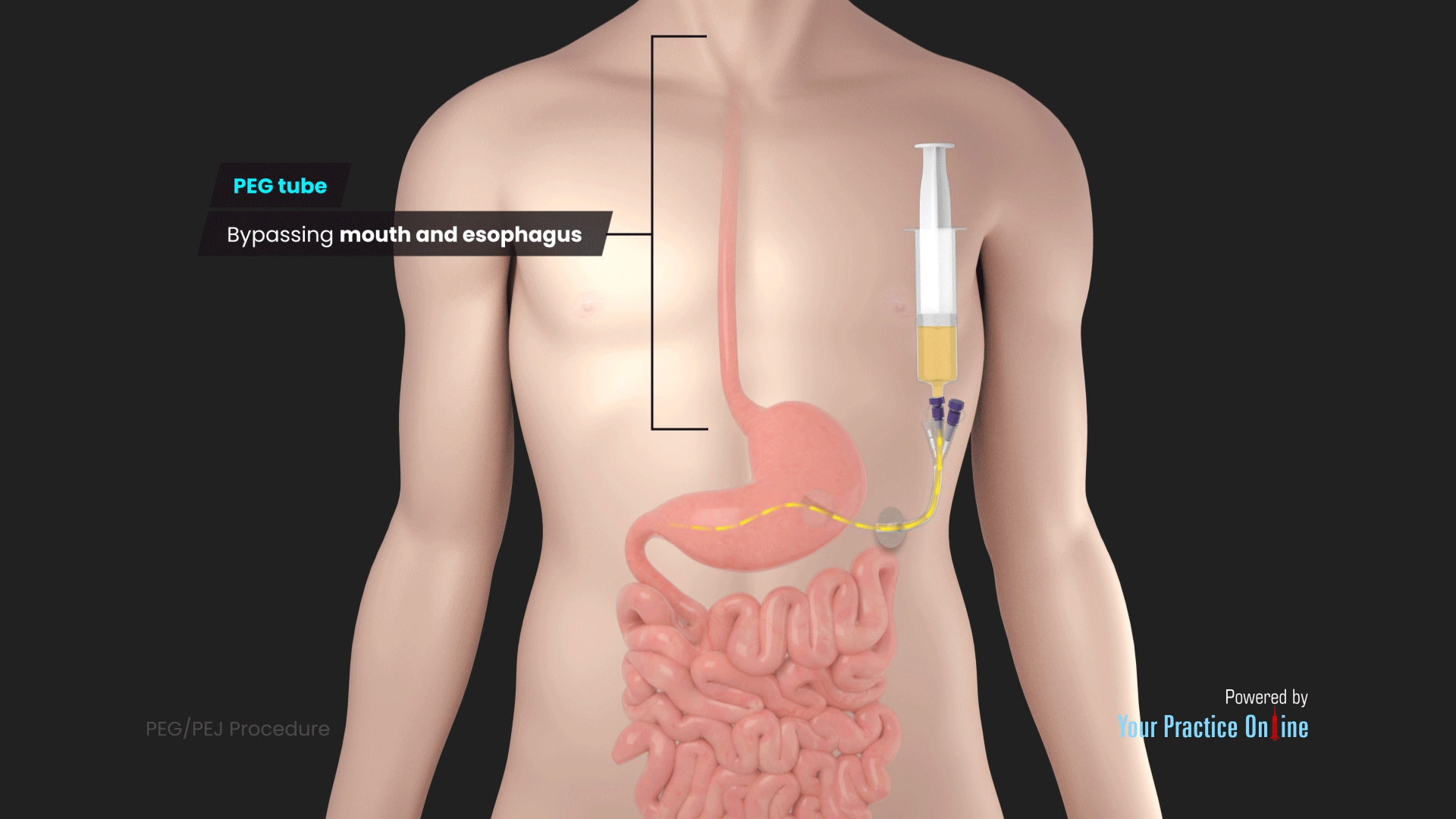
We typically check this by using a syringe attached to the feeding tube. We gently pull back on the syringe, and whatever comes out is the GRV. Easy peasy, right? Well, maybe not always easy peasy, but that’s the gist of it.
Why Do We Even Bother Checking GRV?
This is the million-dollar question, isn't it? Why go through the mild inconvenience of pulling out fluid from a tube when we could just be pumping in more food? Great question! Here are the key reasons:
- Preventing Aspiration: This is probably the BIGGEST reason. If there’s too much fluid sitting in the stomach, it’s more likely to come back up (reflux) and potentially go into the lungs. This is called aspiration, and it can lead to serious problems like pneumonia. Checking GRV helps us gauge the risk.
- Ensuring Tolerance of Feedings: If someone’s stomach is already full and not emptying properly, adding more formula can lead to discomfort, nausea, vomiting, and diarrhea. It’s like trying to cram more stuff into an already overflowing suitcase – it’s just not going to work well.
- Monitoring Gastric Motility: The stomach’s ability to move food along is called gastric motility. Consistently high GRVs can be a sign that the stomach isn’t moving things along as it should. This can alert healthcare providers to potential issues that need further investigation.
- Optimizing Nutrition Delivery: The whole point of tube feeding is to provide adequate nutrition. If we’re constantly dealing with high GRVs and having to hold feedings, the person might not be getting enough calories and nutrients. So, monitoring helps us adjust the feeding plan for better outcomes.
So, you see, it’s not just a random nursing task. It’s a protective measure. It's about making sure the person is comfortable, safe, and actually absorbing the nourishment they're supposed to be getting.
So, What’s the "Normal" Number? The Elusive "Ideal" GRV
Ah, the million-dollar question. And here’s where things get… well, a little less black and white and a lot more shades of gray. Because, to be perfectly honest, there isn't a single, universally agreed-upon “normal” GRV number that applies to everyone, every single time. Shocking, I know!
If you’ve looked at any guidelines or protocols, you might have seen numbers like 200 mL or 250 mL pop up. These have been commonly used thresholds. If the GRV is above these numbers, the thinking was to hold the feeding and notify the healthcare provider.
However, the medical world is always evolving, and research has shown that these old, fixed thresholds might not be the best way to go for everyone. Why? Because people are different! Their stomachs are different. Their conditions are different. What might be perfectly fine for one person could be problematic for another.
The Shift in Thinking: From Fixed Numbers to Individualized Assessment
This is where it gets really interesting, and frankly, a lot more sensible. Instead of blindly sticking to a number, healthcare providers are now encouraged to look at the whole picture.
Think about it: if a person consistently has a GRV of, say, 220 mL, but they are tolerating their feedings well, not experiencing any discomfort, nausea, or vomiting, and their overall condition is stable, is that 220 mL really a problem? Probably not.
On the other hand, if someone has a GRV of 150 mL, but they are actively feeling nauseous, bloated, and retching, then that 150 mL is a significant indicator that something is up.

So, the trend is moving towards a more individualized and clinical approach. This means considering:
- The patient's signs and symptoms: Are they reporting discomfort? Are they vomiting? Are they showing other signs of intolerance?
- The patient's medical history and condition: Some conditions inherently affect gastric emptying more than others.
- The rate and volume of the feeding: A higher feeding rate might naturally lead to a slightly higher GRV.
- The type of formula being used: Some formulas are thicker and might be tolerated differently.
- Trends over time: Is the GRV suddenly higher than it usually is for this patient? Or is it consistently high?
Essentially, we're moving away from a rigid "if it's over X mL, stop" mentality to a more nuanced "let's assess what this GRV means for this specific patient right now."
What About Those Old Guidelines? Are They Totally Useless?
Not necessarily. Those older, more fixed guidelines (like the 200-250 mL cutoffs) can still serve as a starting point or a red flag, especially in certain situations or for certain patient populations where aspiration risk is very high. They can be a useful reminder to be extra vigilant.
However, relying solely on them without considering the patient's overall status is becoming less and less common. Many hospitals and healthcare systems have updated their protocols to reflect this more individualized approach. It’s all about using clinical judgment.
And let’s not forget the patient's comfort! If a GRV is high and the patient is clearly uncomfortable, even if it’s below some arbitrary number, it’s still a reason to investigate and intervene. We’re not just managing numbers; we’re caring for people.
When Do We Check GRV? The Usual Suspects
While the "normal" number might be a bit fluid, the decision of when to check it is usually pretty consistent. The most common times include:
- Before intermittent or bolus feedings: This is the classic scenario. You're about to give a planned dose of formula, so you check what's already there.
- Every 4 to 6 hours for continuous feedings: If someone is receiving a continuous drip of formula, it's often recommended to check GRV at set intervals to ensure ongoing tolerance.
- If the patient shows signs of intolerance: This is crucial. If your patient starts feeling sick, nauseous, or is vomiting, checking the GRV is a priority, regardless of the scheduled time.
- After a change in feeding regimen: If the rate, volume, or type of formula is changed, it's wise to monitor the GRV more closely initially.
It’s also worth noting that the frequency and specific protocol for checking GRV can vary depending on the patient's condition, the type of feeding tube, and the healthcare facility’s policies. Always, always, always follow your facility’s specific guidelines and the doctor's orders.
What If the GRV is High? What Happens Next?
Okay, so you’ve done the check, and the GRV is higher than you expected, or higher than the current guideline suggests. What now? Don't panic! This is where your critical thinking skills come into play.
First, as we discussed, assess the patient. Are they in distress? Any signs of nausea, vomiting, abdominal distension (a swollen belly), or pain?
Generally, if the GRV is high and the patient is asymptomatic (meaning they have no symptoms), some protocols might suggest rechecking it after an hour to see if it decreases. If it remains high, or if the patient is symptomatic, the usual steps are:
- Hold the next feeding: You don't want to add more fuel to the fire.
- Notify the healthcare provider: This is the most important step. The doctor or advanced practice provider needs to know. They will evaluate the situation.
- Further assessment and potential interventions: The healthcare provider might order tests to look for underlying issues with gastric emptying, adjust medications, change the feeding formula, or alter the feeding regimen (e.g., slow down the rate, decrease the volume).
Sometimes, especially if the GRV is extremely high, the collected gastric contents might be sent to the lab for analysis. This can provide valuable information.
Remember, the goal isn't just to "fix" a high number; it's to understand why it's high and to ensure the patient's safety and well-being.
Tips and Tricks for Measuring GRV (From One Human to Another)
Let’s get a little practical, shall we? Because sometimes, the actual act of checking GRV can be… interesting.
- Be gentle: Always pull back on the syringe slowly and gently. You don’t want to traumatize the stomach lining or cause unnecessary discomfort.
- Use the right size syringe: Usually, a 60 mL syringe is recommended. Smaller syringes can create too much negative pressure.
- Prime the tube first: Some facilities recommend flushing the tube with a small amount of water (e.g., 10-30 mL) before attempting to aspirate the GRV. This can help dislodge any thick formula and make aspiration easier. Always check your facility's protocol for this.
- Don't force it: If you can't get anything back, don't keep yanking on the syringe. It might mean the tube is kinked, clogged, or positioned incorrectly.
- Document everything: Record the amount of GRV obtained, the patient's tolerance, and any interventions. This is crucial for tracking progress and for communication.
- When in doubt, ask! Seriously, no one expects you to know everything. If you're unsure about a GRV measurement or what to do, ask a more experienced colleague or your supervisor. It’s better to ask than to guess.
And here’s a little anecdote for you: I once had a patient whose GRVs were always through the roof. We tried everything – slowing down feedings, changing formulas, all the usual tricks. Turns out, they had a very advanced form of gastroparesis, and their stomach was just… slow. Once we understood that, we could adjust the feeding plan and focus on managing their symptoms, rather than just chasing a number. It was a good reminder that the numbers are just clues; the patient is the one who holds the real story.
The Bottom Line: GRV is a Tool, Not the Whole Story
So, there you have it. Gastric residual volume – no longer a scary, mysterious medical term, but a practical tool used to ensure safe and effective tube feeding.
While there used to be rigid numbers, the trend is decidedly towards a more patient-centered, individualized approach. We look at the GRV in conjunction with the patient’s overall condition, their symptoms, and their medical history.
It's about using our clinical judgment, listening to our patients, and working as a team to provide the best possible care. The GRV is just one piece of the puzzle, but it's an important one in helping us keep our patients safe, comfortable, and well-nourished.
Next time you hear about GRV, I hope you’ll feel a little more confident and a lot less anxious. It’s just another way we care for people, making sure they get the support they need to heal and thrive. Keep asking questions, keep learning, and you’ll be a GRV guru in no time!